

I find it hard to believe that there is too little information one could get about Davao Regional Hospital in the internet, considering its popularity among the people of Davao and its wide service coverage in terms of land area. I can't even find its logo using Google Search. All we could see are pictures of DRH in the past. What about now? Our hospital has evolved for the better. It's about time to upload new and improved photos of DRH. It's about time to extend the services that DRH can offer through the cyber-space.
The official DRH website is yet to be finished. Until then, with the permission of our superiors, we will be providing relevant and up-to-date information about DRH through the World Wide Web with the use of this blogspot. A.K.A. Angels in the Sickroom; (a web-based information site about the Davao Regional Hospital and other topics related to healthcare).
Explore the Angels in the Sickroom site and access the following features:
• CHAT – get in touch with friends here and abroad through chat box
• SITEMAP – zoomable aerial view image of the Davao Regional Hospital
• ABOUT DRH
• VISION + MISSION of DRH
• ORGANIZATIONAL STRUCTURE of DRH
• UPDATES + ANNOUNCEMENTS
• PHOTO ALBUM – pictures of DRH and more
• LEARN – facts about healthcare and more
• DOWNLOAD – free source of downloadable files by request
Our goal is to be able to provide accurate and useful data related to healthcare, medicine, diagnostics and comptech support based on the demands of those who thirst for more knowledge. To date, Angels in the Sickroom is still in the development phase. More features will be added to cater to the needs of its visitors or readers as the development goes on. Our future posts or topics will be based on your demands dear readers and subscribers. Feel free to send in your requests through the provided chat box. Comments and suggestions are also encouraged.
The website administrator is also in need of content contributors for this blogspot. Share your knowledge and skills through Angels in the Sickroom by contributing educational articles, news, facts, photos, softwares and other useful multimedia files. To start sharing now, please contact the technical support team or e-mail your desire to become a content contributor to D5NSS1L@GMAIL.COM.
FAST AND SECURE
SIGN UP NOW FOR FREE

Wednesday, October 20, 2010
LEARN ALL YOU CAN
Explore this blogspot and know more about normal values, coronary care, healthy diet, ECG, and more.
Click HERE to start learning now.
Click HERE to start learning now.
Monday, August 9, 2010
DAVAO REGIONAL HOSPITAL INFORMATION TECHNOLOGY TRAINING CENTER
The Davao Regional Hospital is in need of a computer-literacy team to prepare DRH employees for the inevitable and essential DRH upgrade through computer technology. Hiring a team of already established computer instructors is an option. However, DRH itself is blessed to have current employees who may be able to handle the job. A single screening session may be enough to identify the appropriate members of the literacy team.
The Hospital Operations and Management Information System; (HOMIS) will soon be launched. It is composed of a variety of programs that will ease-up hospital operations and patient management. The best way to prepare DRH is to activate the proposed Information Technology Training Center in Davao Regional Hospital the soonest time possible.
The extent of the preliminary computer operation instructions that will be rendered by the newly organized computer-literacy team will depend on the launch date of the first program of HOMIS. The first HOMIS component / program that will be activated is the Ward Module. The said program will serve as the ultimate solution to problems pertaining to hospital charges and patient data management. (Please refer to Ward Module Objectives and Guidelines for details).Basic computer operation may be taught prior to the actual operation of the first HOMIS component if time permits. This is to maximize the transfer of knowledge during each instruction session and to prevent re-instruction of basic computer operation whenever another HOMIS component will be introduced.
In case of shortage of time, the instructors shall study the Ward Module and identify the basic computer operations that are necessary in the actual operation or manipulation of the said HOMIS program. Immediately after each instruction session the end-users shall be able to startup the computer, launch HOMIS, activate Ward Module, input correct data, save files, retrieve files, identify problems and solutions, exit HOMIS safely, shutdown the computer safely, and know who to call when problems arise.
Aside from the ever reliable and functional IHOMP of DRH, the computer-literacy team may be composed of representatives from the key departments of DRH such as the administrative, medical, nursing, laboratory, and ancillary departments in order to facilitate a more effective transfer of knowledge. This strategy will also take into account the advantage brought about by immersion to the key areas of DRH. The employees who are immersed in the clinical and special areas for quite some time will be able to identify the problems encountered by DRH employees that can be solved with the utilization of computer technology. They will also be able to contribute to the development of HOMIS programs and other simple solutions to the said problems through information technology. One example of the said simple solutions would be the Virtual Kardex. The developer of the said program aims to eliminate the traditional method of end-of-shift-reports among nurses and facilitate a better and faster endorsement of patients and patient management to ensure a more efficient continuity of patient care. Virtual Kardex is still in the development and enhancement stage and is now open for evaluation and trial. The other key departments of DRH may have been experiencing problems and are thinking of ways to eliminate the said problems through information technology. Now is the right time to develop and enhance solutions that can possibly be incorporated in the very efficient DRH informatics tool that is…HOMIS.
The Hospital Operations and Management Information System; (HOMIS) will soon be launched. It is composed of a variety of programs that will ease-up hospital operations and patient management. The best way to prepare DRH is to activate the proposed Information Technology Training Center in Davao Regional Hospital the soonest time possible.
The extent of the preliminary computer operation instructions that will be rendered by the newly organized computer-literacy team will depend on the launch date of the first program of HOMIS. The first HOMIS component / program that will be activated is the Ward Module. The said program will serve as the ultimate solution to problems pertaining to hospital charges and patient data management. (Please refer to Ward Module Objectives and Guidelines for details).Basic computer operation may be taught prior to the actual operation of the first HOMIS component if time permits. This is to maximize the transfer of knowledge during each instruction session and to prevent re-instruction of basic computer operation whenever another HOMIS component will be introduced.
In case of shortage of time, the instructors shall study the Ward Module and identify the basic computer operations that are necessary in the actual operation or manipulation of the said HOMIS program. Immediately after each instruction session the end-users shall be able to startup the computer, launch HOMIS, activate Ward Module, input correct data, save files, retrieve files, identify problems and solutions, exit HOMIS safely, shutdown the computer safely, and know who to call when problems arise.
Aside from the ever reliable and functional IHOMP of DRH, the computer-literacy team may be composed of representatives from the key departments of DRH such as the administrative, medical, nursing, laboratory, and ancillary departments in order to facilitate a more effective transfer of knowledge. This strategy will also take into account the advantage brought about by immersion to the key areas of DRH. The employees who are immersed in the clinical and special areas for quite some time will be able to identify the problems encountered by DRH employees that can be solved with the utilization of computer technology. They will also be able to contribute to the development of HOMIS programs and other simple solutions to the said problems through information technology. One example of the said simple solutions would be the Virtual Kardex. The developer of the said program aims to eliminate the traditional method of end-of-shift-reports among nurses and facilitate a better and faster endorsement of patients and patient management to ensure a more efficient continuity of patient care. Virtual Kardex is still in the development and enhancement stage and is now open for evaluation and trial. The other key departments of DRH may have been experiencing problems and are thinking of ways to eliminate the said problems through information technology. Now is the right time to develop and enhance solutions that can possibly be incorporated in the very efficient DRH informatics tool that is…HOMIS.
Monday, May 3, 2010
ECG
CLICK HERE TO RUN ONLINE ECG SIMULATOR
CLICK HERE TO DOWNLOAD OFFLINE ECG SIMULATOR
______________________________________________
POWERED BY: SkillStat Learning + 4shared + Photobucket
MOST COMMON ECGs:
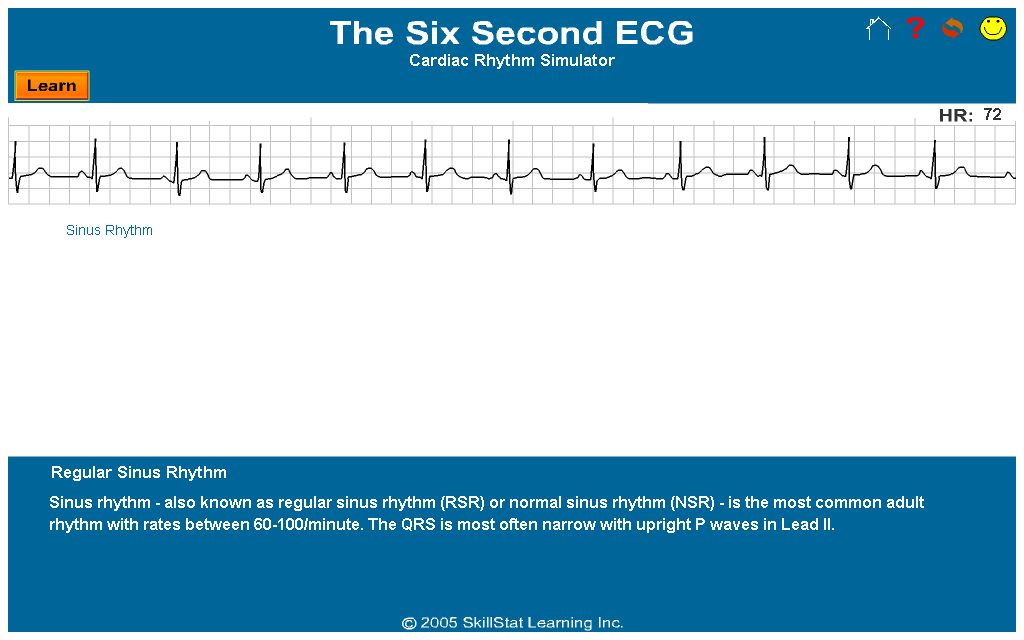
SINUS RHYTHM
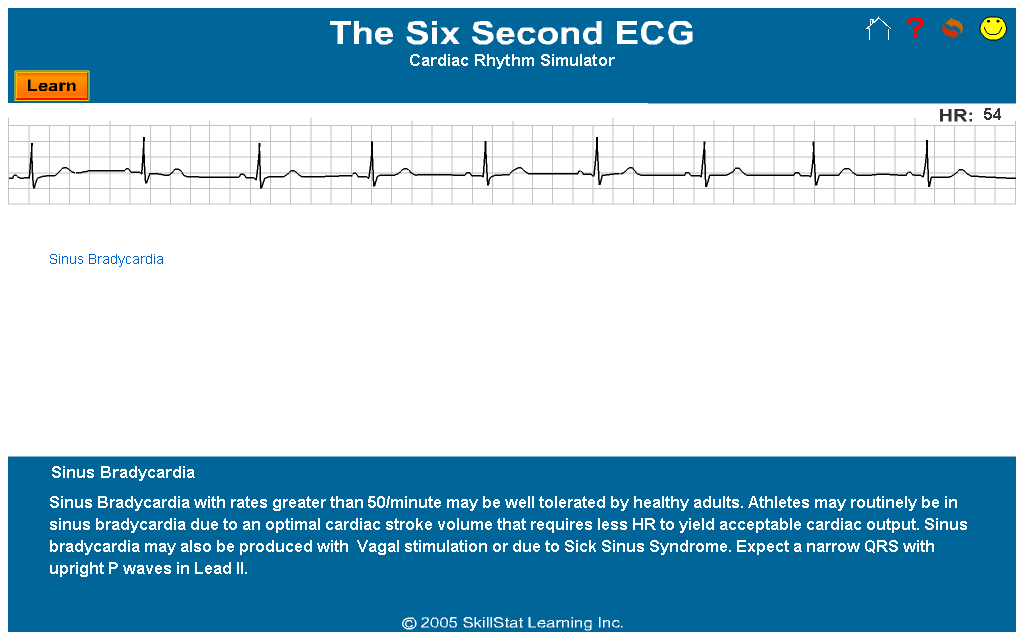
SINUS BRADYCARDIA
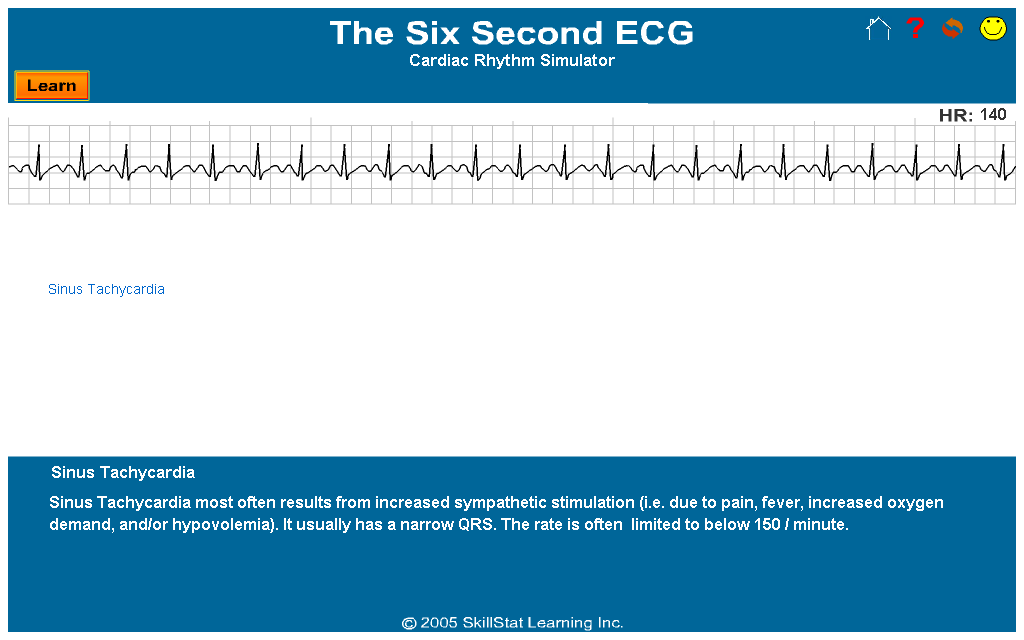
SINUS TACHYCARDIA
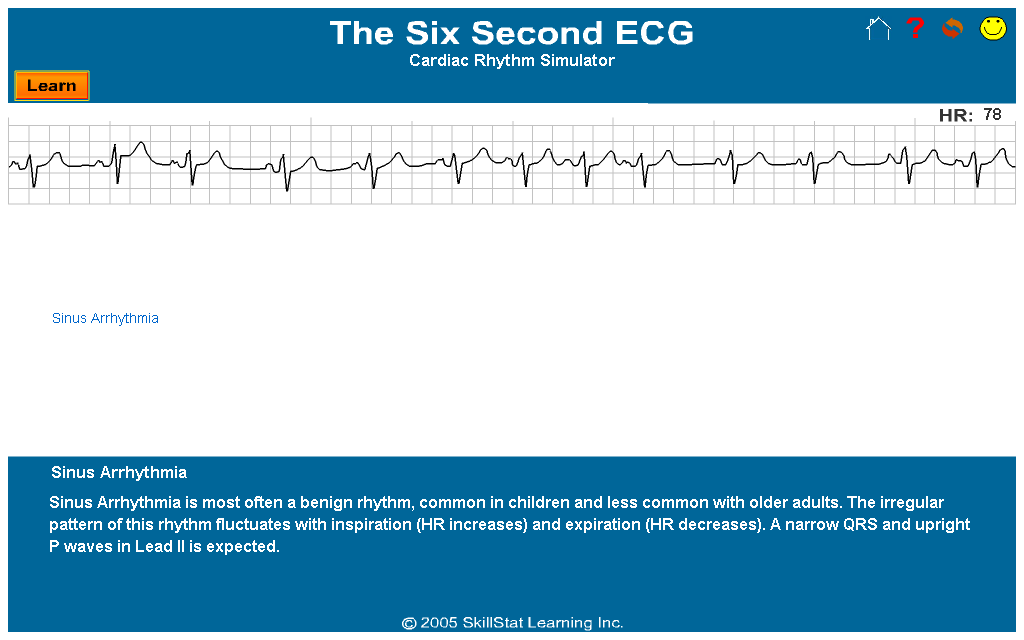
SINUS ARRHYTHMIA
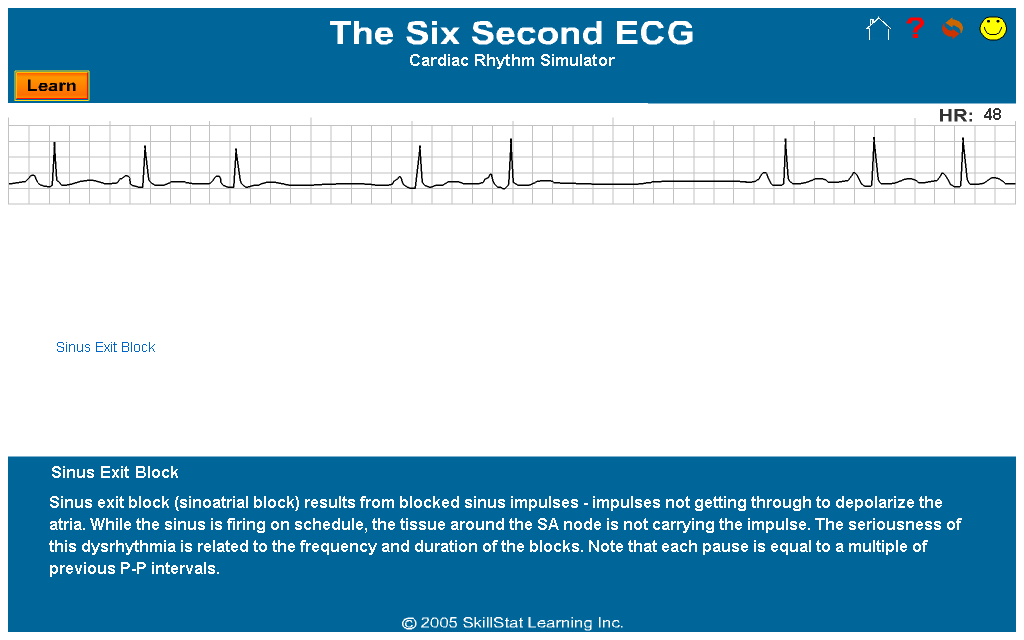
SINUS EXIT BLOCK
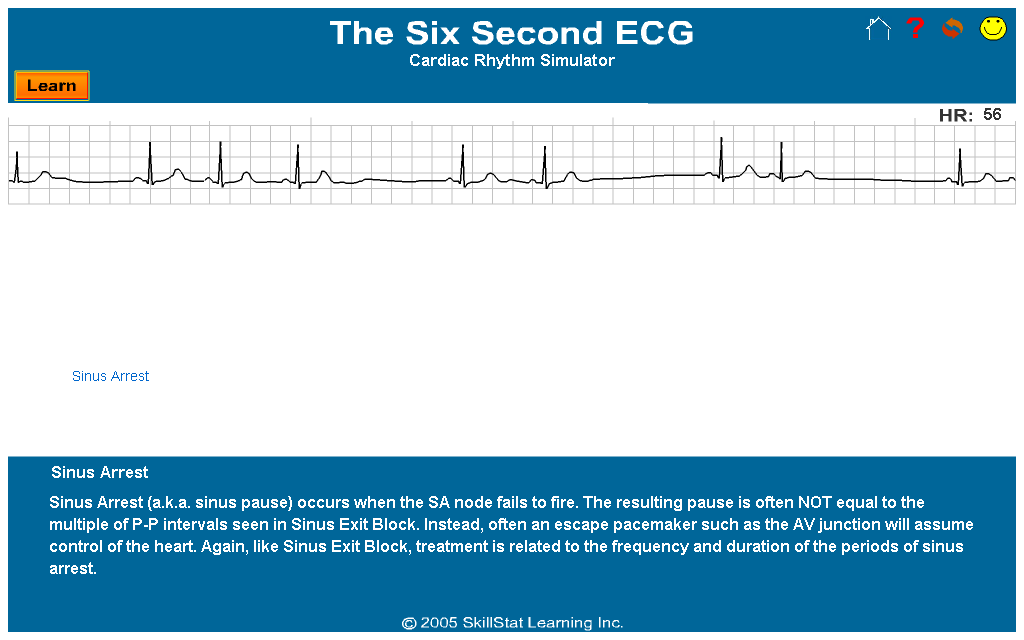
SINUS ARREST
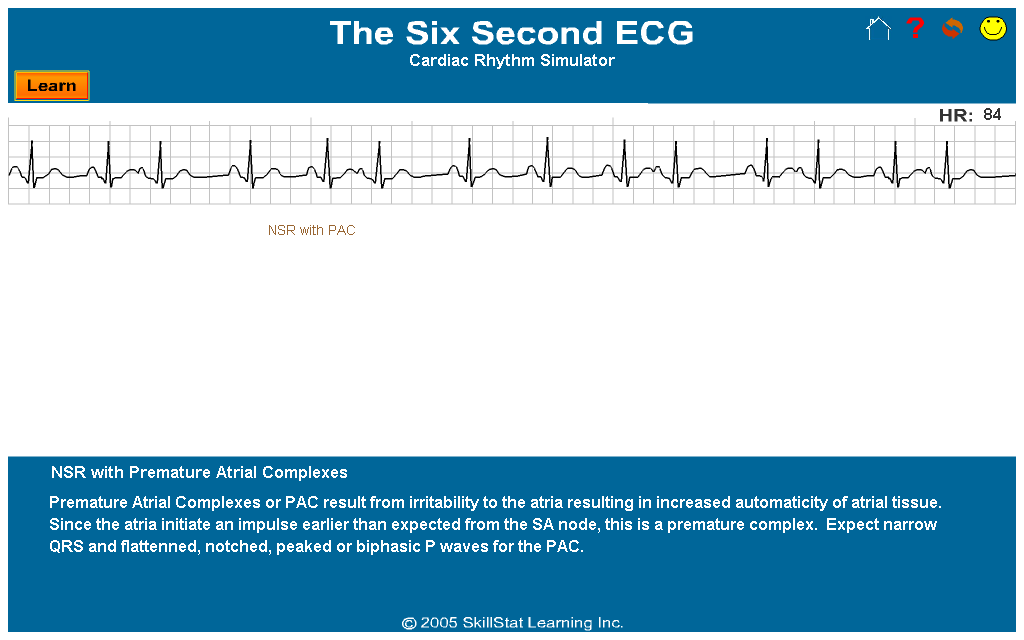
NSR WITH PAC
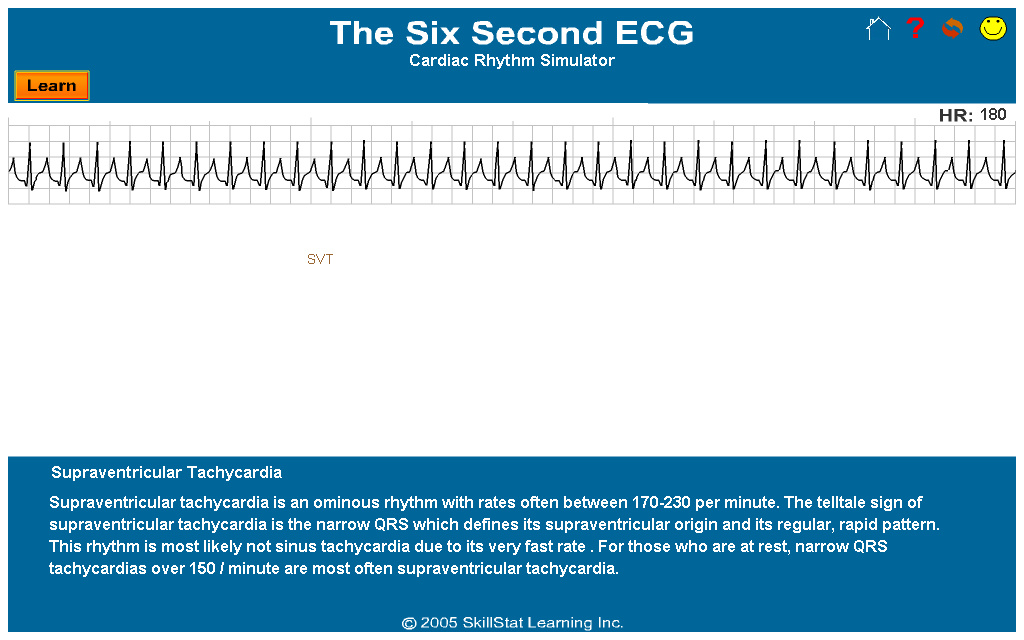
SVT
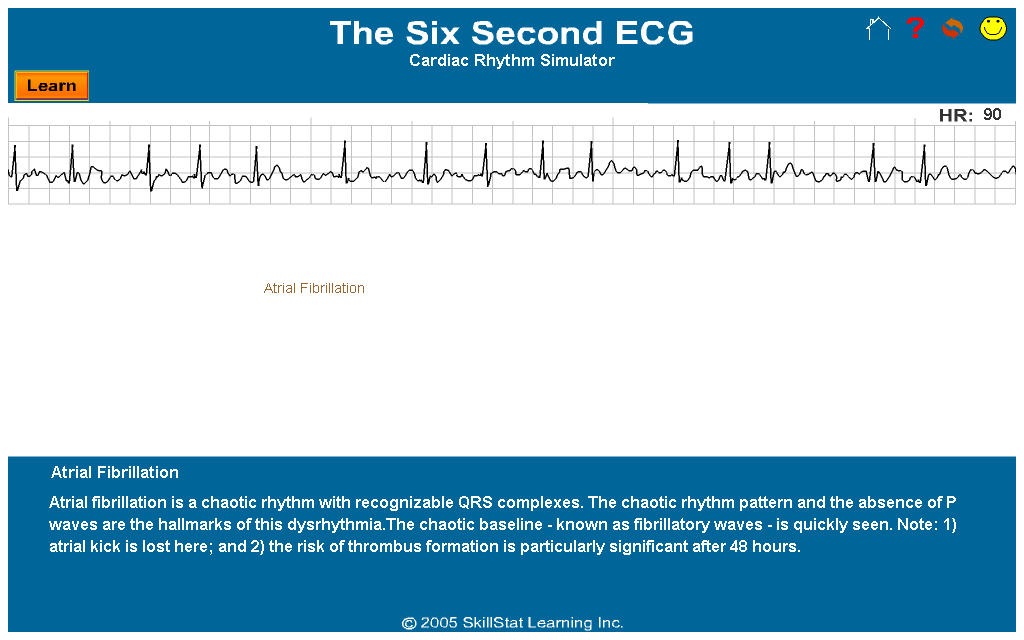
ATRIAL FIBRILLATION
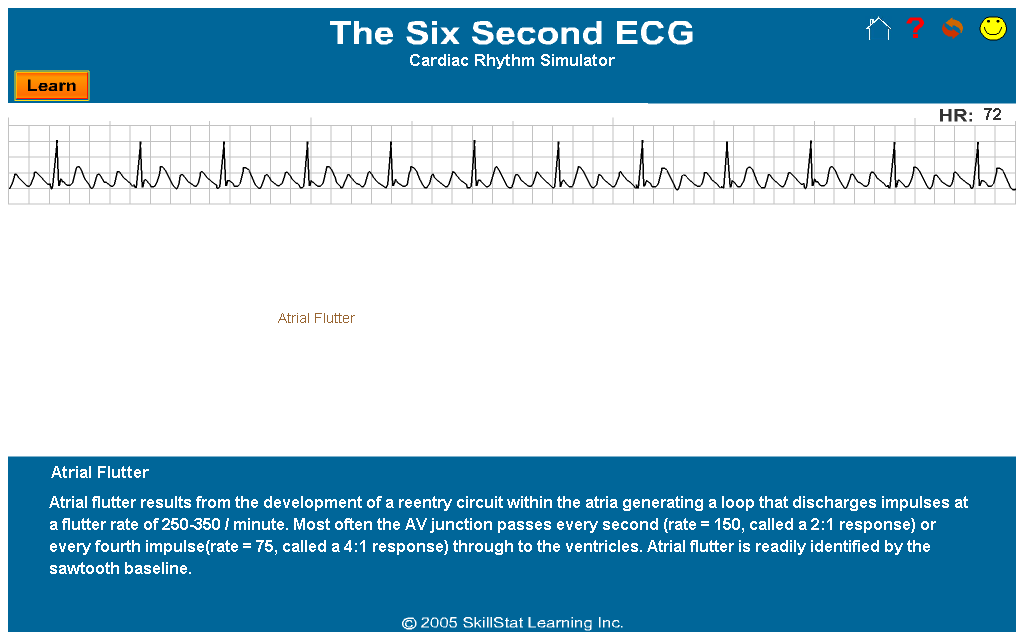
ATRIAL FLUTTER
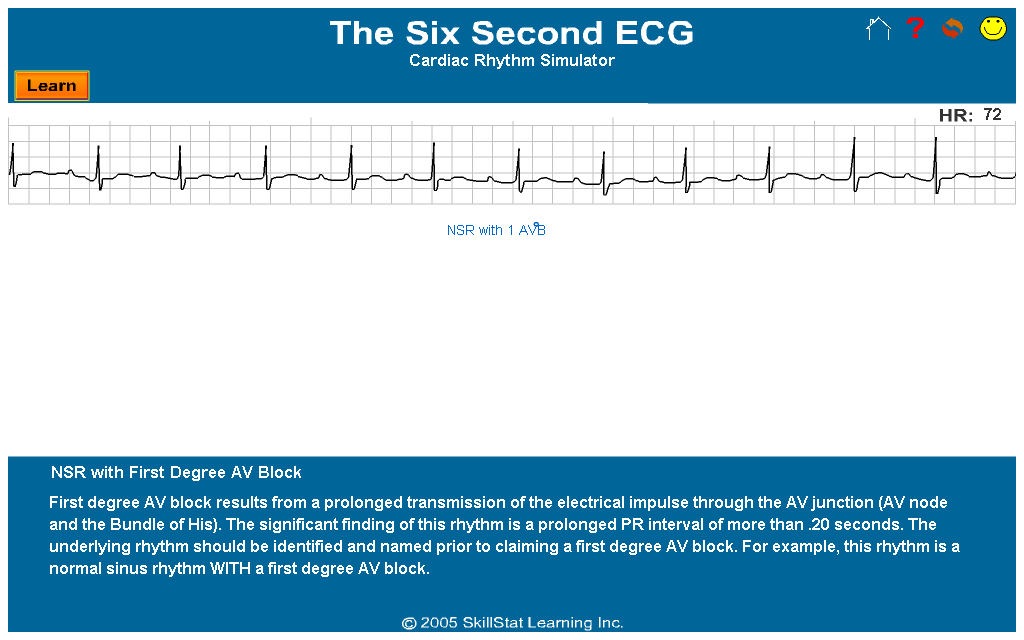
NSR WITH FIRST DEGREE AV BLOCK
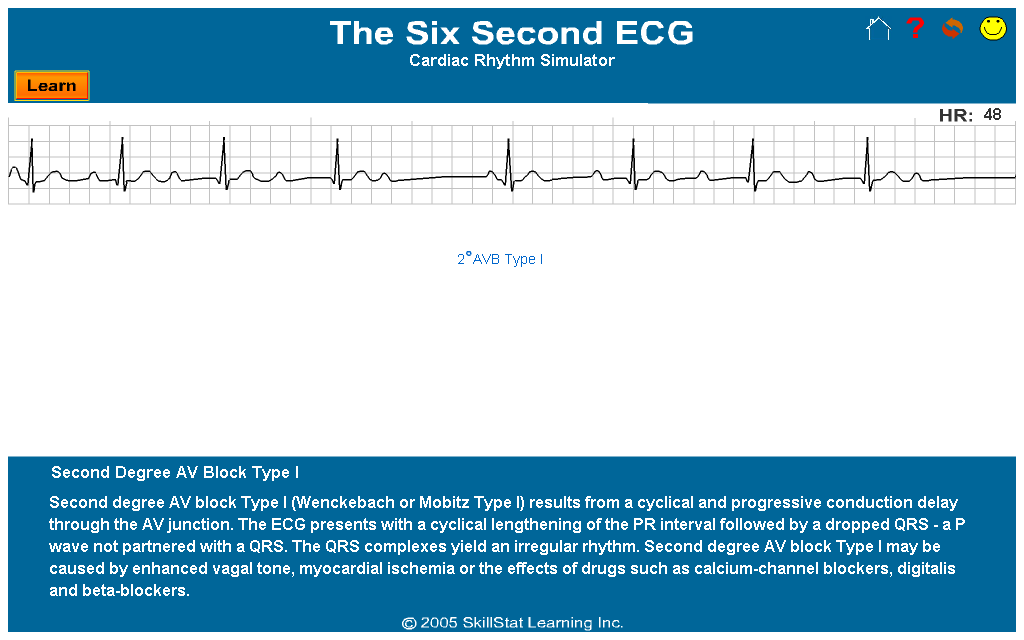
SECOND DEGREE AV BLOCK TYPE I
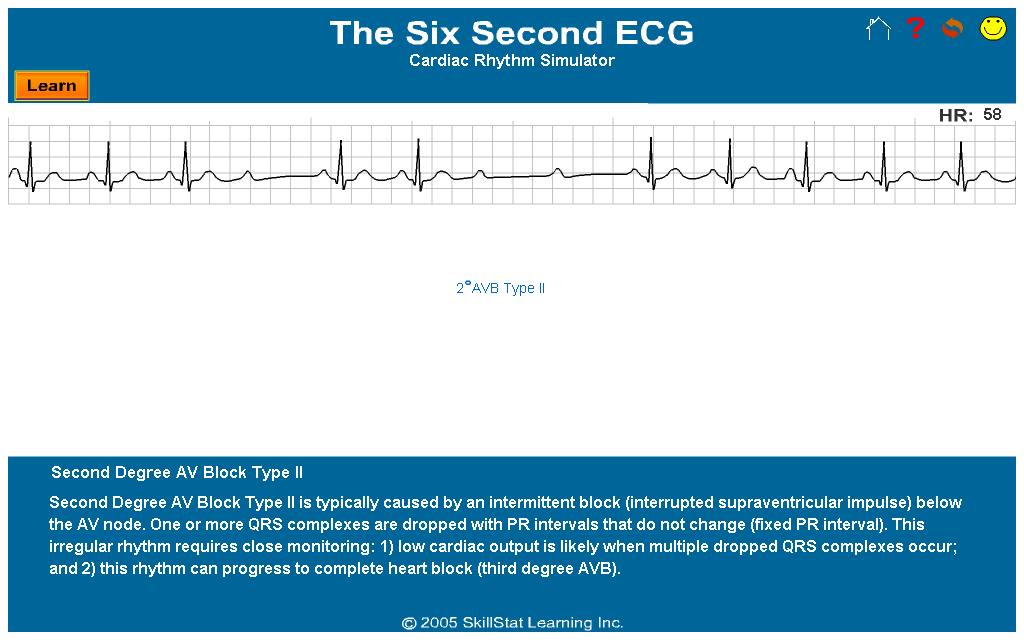
SECOND DEGREE AV BLOCK TYPE II
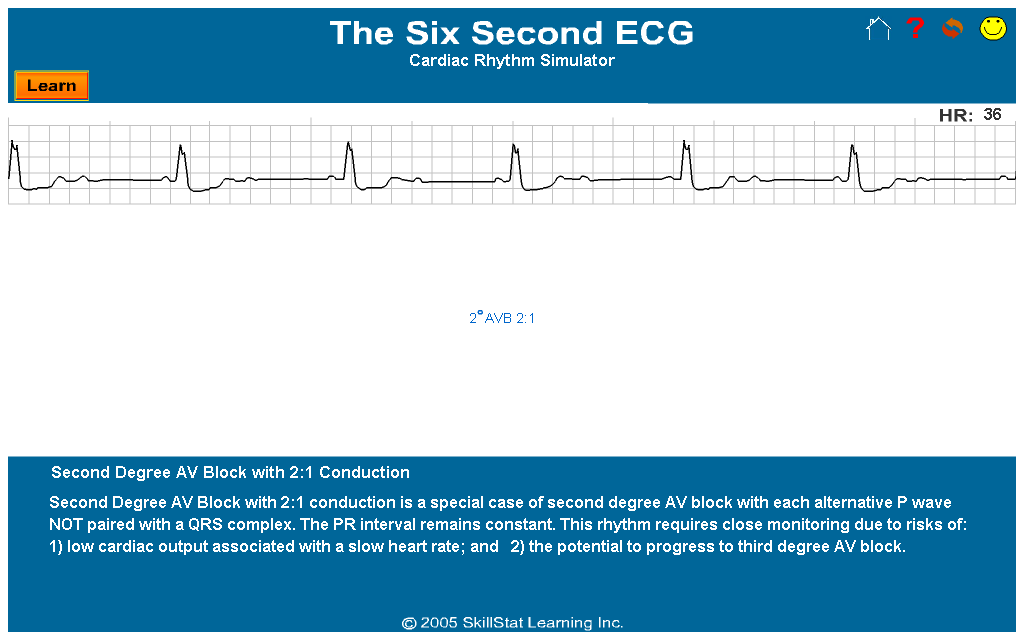
SECOND DEGREE AV BLOCK 2:1
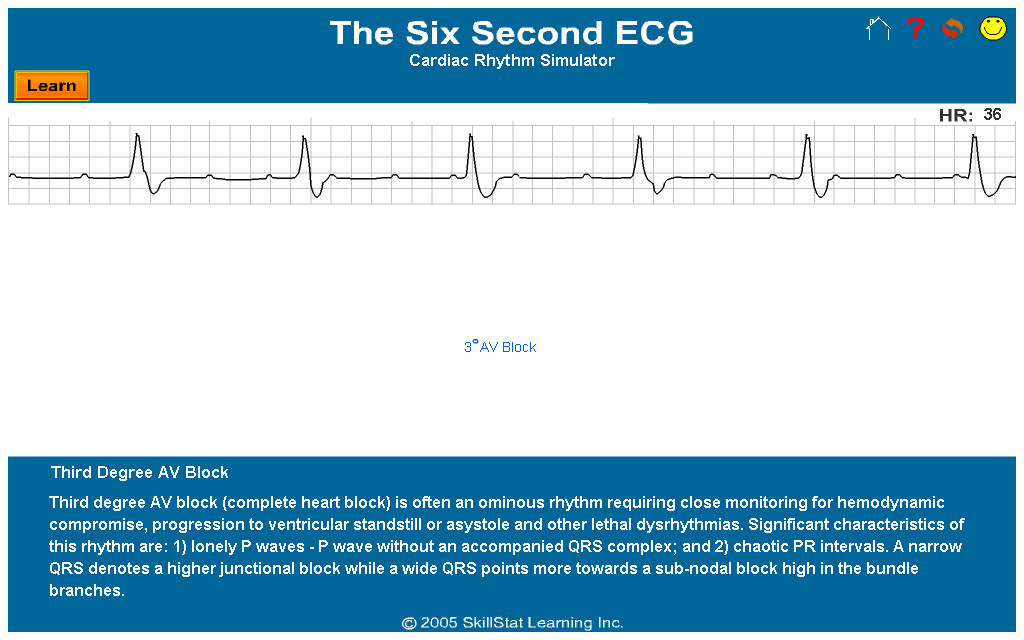
THIRD DEGREE AV BLOCK
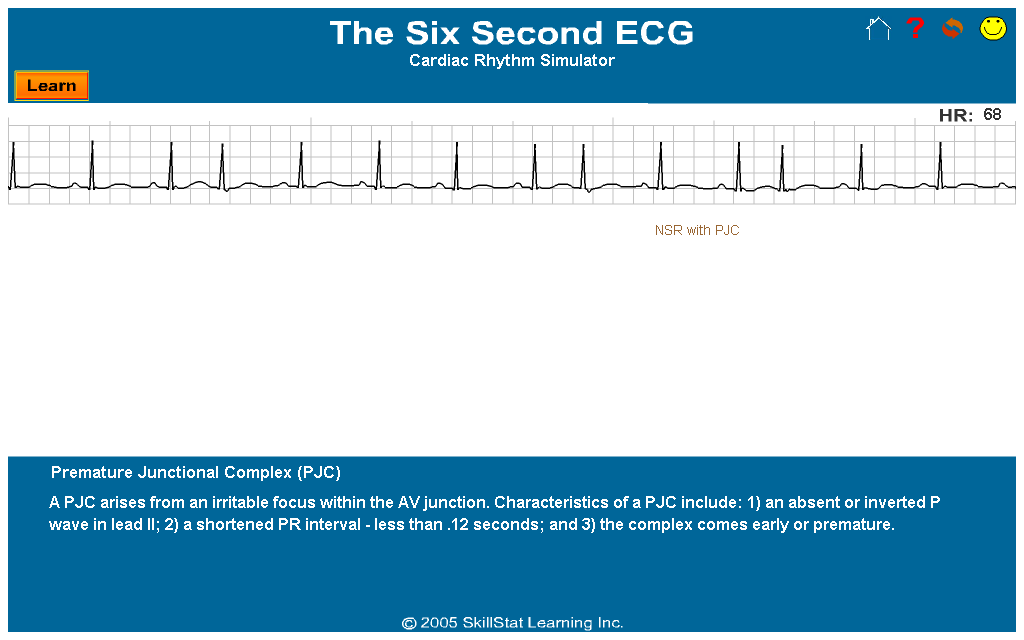
NSR WITH PJC
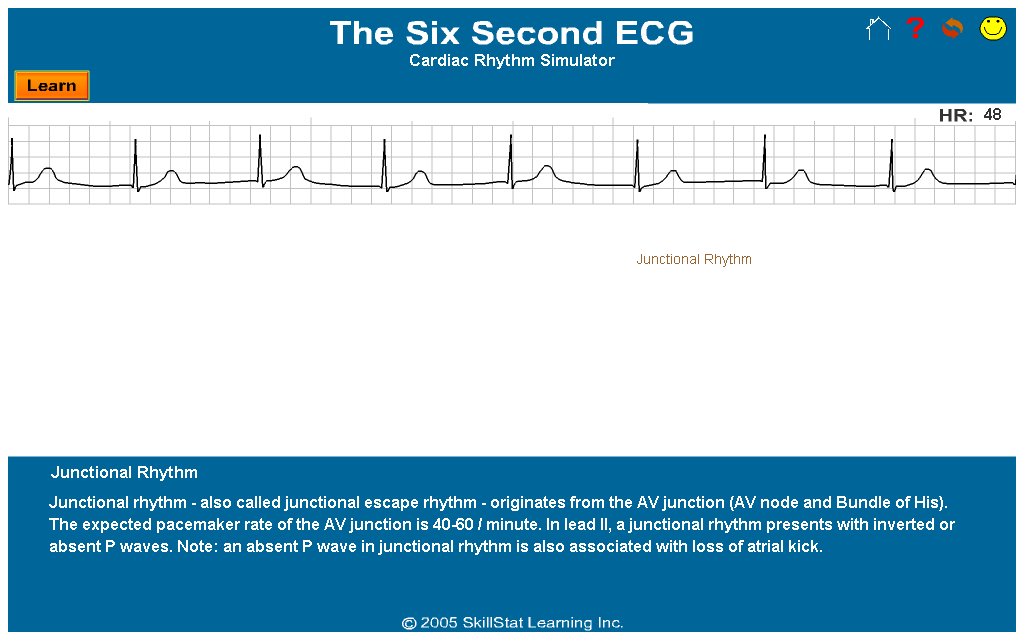
JUNCTIONAL RHYTHM
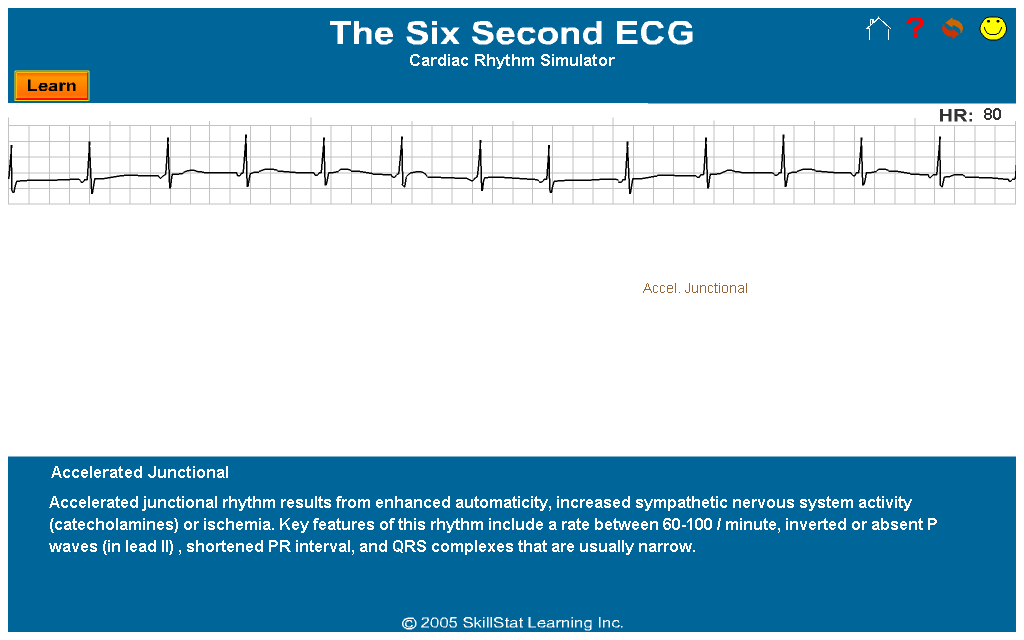
ACCELERATED JUNCTIONAL
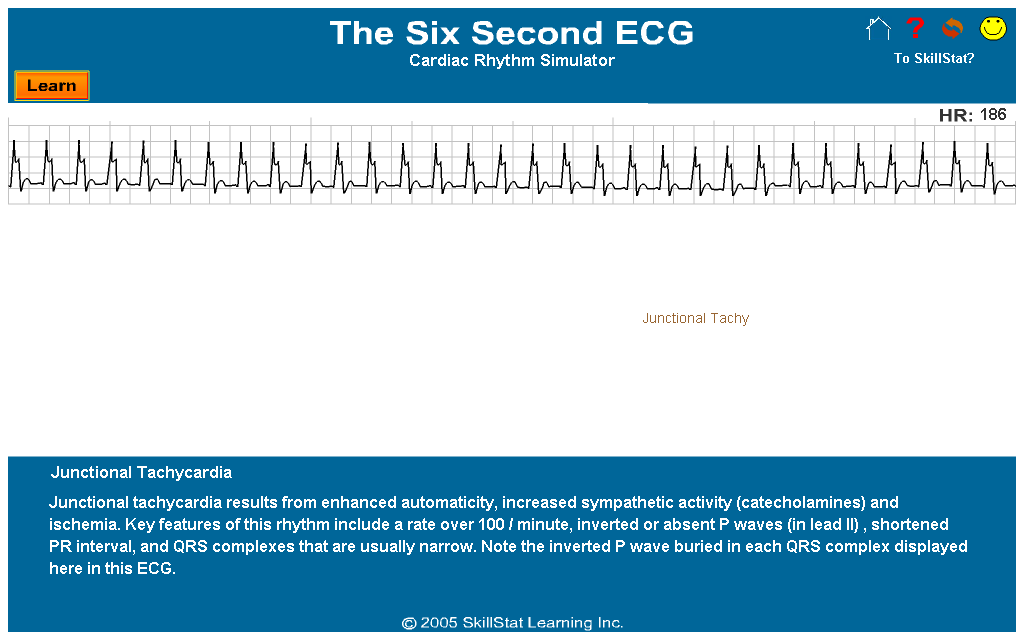
JUNCTIONAL TACHYCARDIA
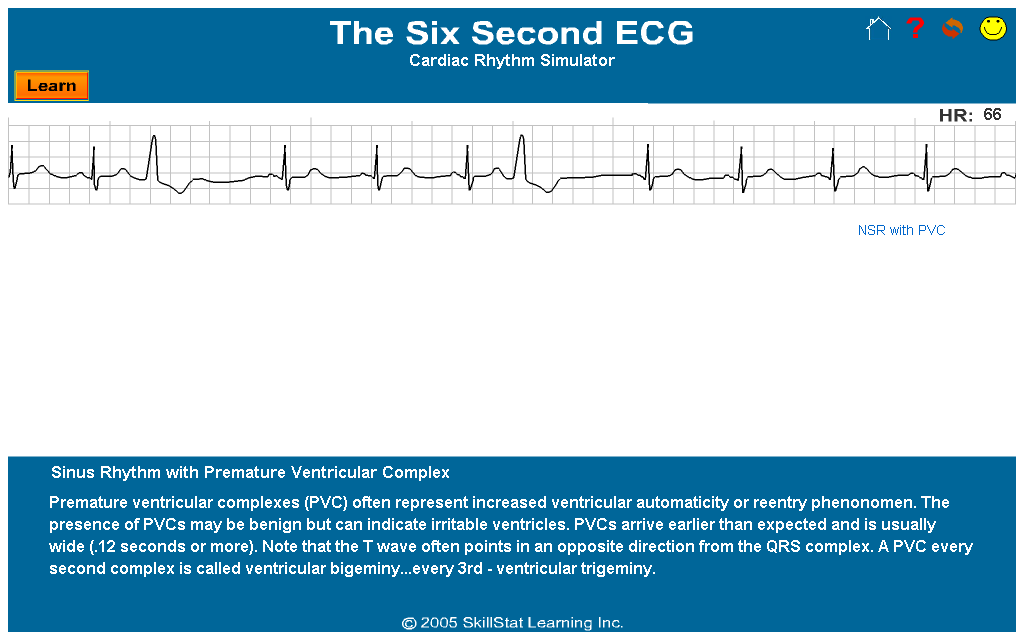
NSR WITH PVC
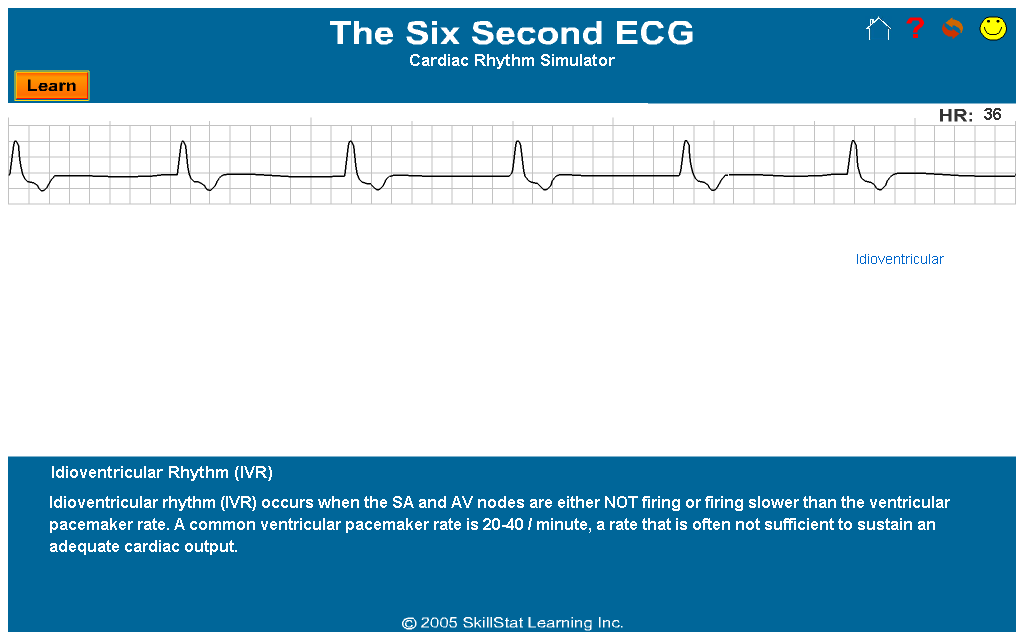
IDIOVENTRICULAR RHYTHM
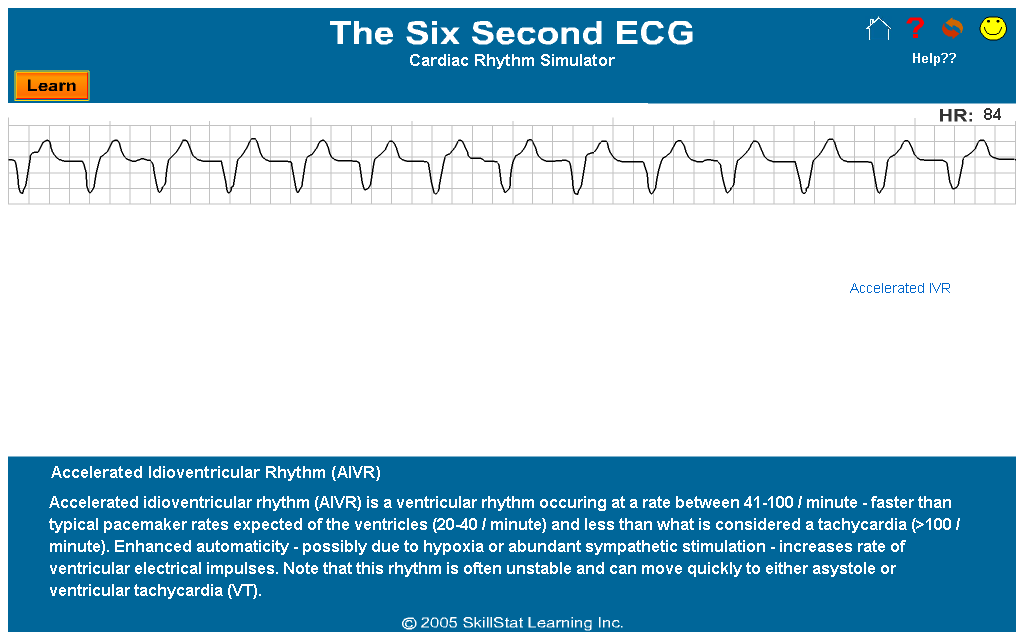
ACCELERATED IDIOVENTRICULAR RHYTHM
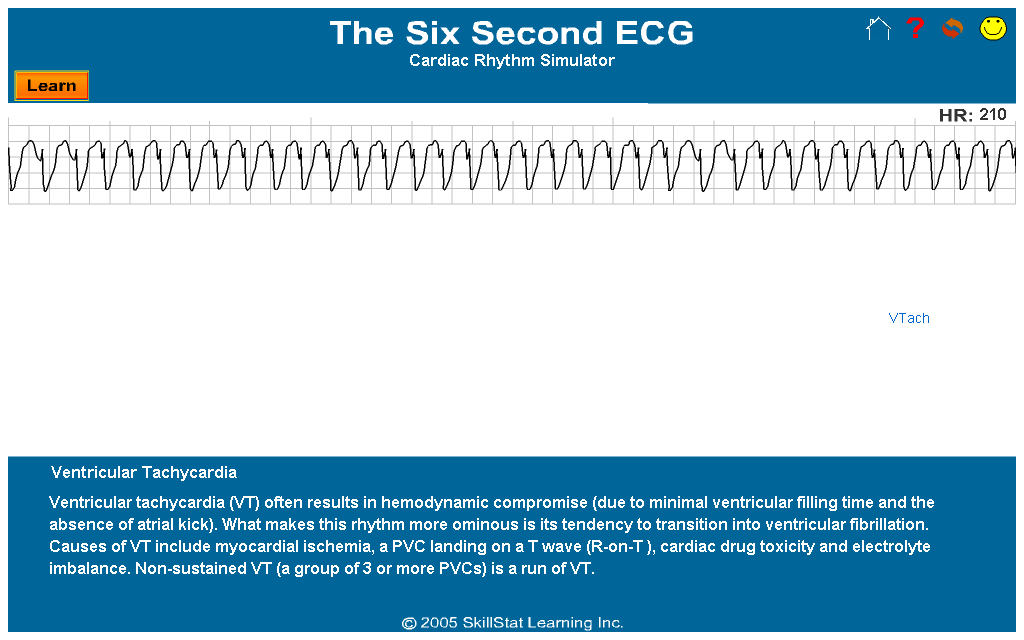
VENTRICULAR TACHYCARDIA
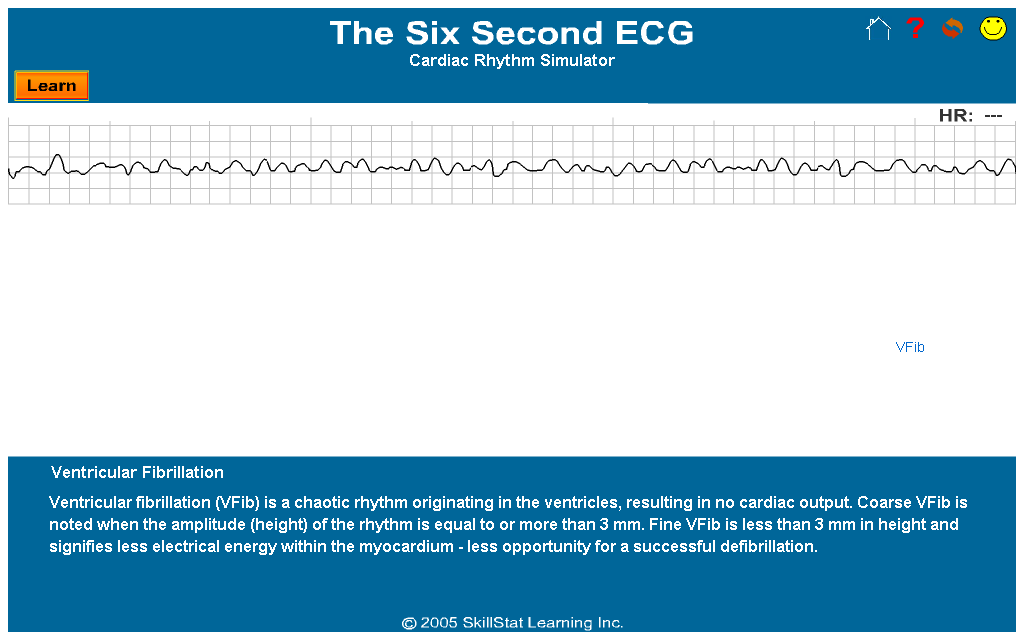
VENTRICULAR FIBRILLATION
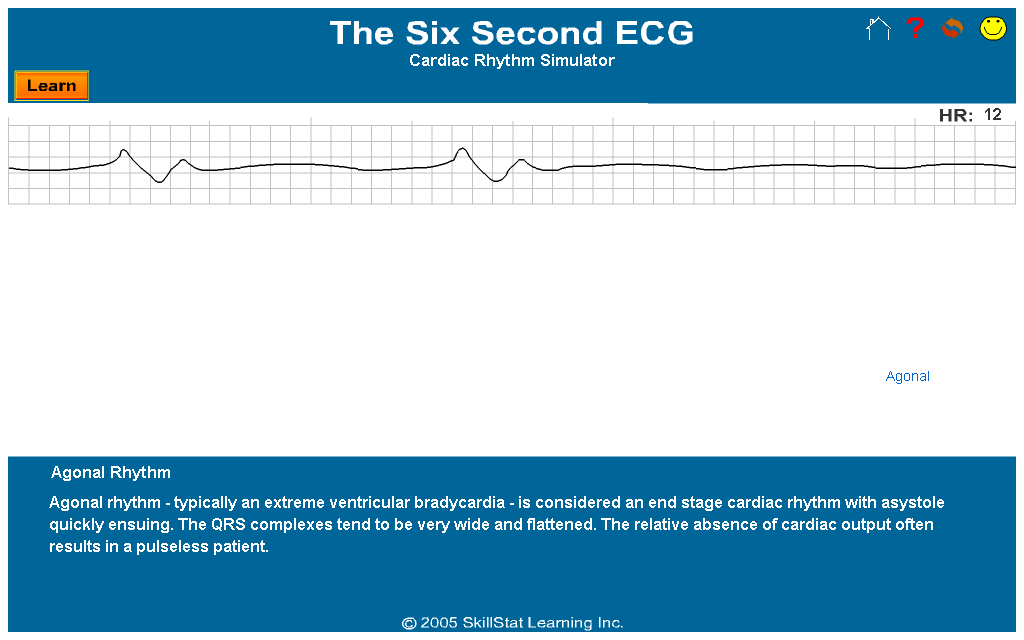
AGONAL RHYTHM
OTHERS:
ACUTE MI
ANTERIOR WALL MI
HYPERKALEMIA
CLICK HERE TO DOWNLOAD OFFLINE ECG SIMULATOR
______________________________________________
POWERED BY: SkillStat Learning + 4shared + Photobucket
MOST COMMON ECGs:
SINUS RHYTHM
SINUS BRADYCARDIA
SINUS TACHYCARDIA
SINUS ARRHYTHMIA
SINUS EXIT BLOCK
SINUS ARREST
NSR WITH PAC
SVT
ATRIAL FIBRILLATION
ATRIAL FLUTTER
NSR WITH FIRST DEGREE AV BLOCK
SECOND DEGREE AV BLOCK TYPE I
SECOND DEGREE AV BLOCK TYPE II
SECOND DEGREE AV BLOCK 2:1
THIRD DEGREE AV BLOCK
NSR WITH PJC
JUNCTIONAL RHYTHM
ACCELERATED JUNCTIONAL
JUNCTIONAL TACHYCARDIA
NSR WITH PVC
IDIOVENTRICULAR RHYTHM
ACCELERATED IDIOVENTRICULAR RHYTHM
VENTRICULAR TACHYCARDIA
VENTRICULAR FIBRILLATION
AGONAL RHYTHM
OTHERS:
ACUTE MI
ANTERIOR WALL MI
HYPERKALEMIA
Sunday, May 2, 2010
CORONARY CARE
Hospital Care And The Coronary Care Unit (CCU)
Most patients suspected of having suffered an acute heart attack are admitted to a hospital's coronary care unit (CCU). The CCU is intended to be a quiet, calm, and restful area in which patients can be further evaluated and closely monitored. A specially trained nurse who works with doctors and other members of the medical team provides individualized care. Visiting hours are usually restricted.
The length of stay in the CCU varies, depending on :
• Whether or not the diagnosis of a heart attack is confirmed
• The severity of the heart attack
• The presence and severity of associated complications
A patient with a heart attack without complications spends about two to three days in a CCU before being transferred to a step-down unit. A step-down unit offers less intensive care than the CCU but still permits continuous ECG monitoring to screen for abnormal heart rhythms or other complications. The patient usually goes home five to seven days after hospital admission.
What Are The Goals Of Care In The CCU?
Care in the CCU focuses on:
• Relief of chest pain and anxiety
• Further assessment (diagnostic tests) to confirm a diagnosis
• Limiting the size of the heart attack and the area of heart muscle that dies
• Reducing the work of the heart
• Identifying, preventing, and treating complications from the heart attack
In the CCU:
• Care for the patient begun in the emergency setting continues
• Additional diagnostic tests are ordered
• Doctors determine appropriate medical-surgical intervention.
• The patient's level of activity and diet is restricted
Diet And Activity Levels
Additional precautions taken during the stay in the CCU and step-down unit, include
• Restricting the diet
For the first 24 hours, the patient is placed on a clear liquid diet to reduce the possibility of aspiration due to nausea and vomiting. A healthy food plan, including complex carbohydrates and fiber-rich foods, is later introduced. All individuals who have suffered a heart attack need to permanently adopt a healthy diet.
• Limiting activity levels
All patients are initially placed on bed rest. Patients who are stable, free of pain, and free of complications are sometimes to get out of bed to use the commode. Patients who remain free of complication often begin limited physical activities within 24 hours.
Progression Of Activity
Days 1-2
• Sitting up with feet dangling over the side of the bed
• Lifting and lowering of the arms, called range-of-motions exercises, to prevent muscle and joint stiffness and to prevent blood clots from forming in the legs
Days 3-4
• Bathing and dressing while sitting on the bed or in a chair
• Taking short walks around the hospital room
• Taking supervised walks outside the hospital room
• Showering without shampooing hair (no raising of arms above head)
Days 5-7
• Walking about 600 feet three times a day
• Shampooing hair (activities with arms over the head)
• Climbing stairs with supervision
• Undergoing an exercise tolerance test
After several days in the hospital, a patient with an uncomplicated heart attack can go home. Physical activity is then gradually increased over the next three to six weeks. Doctors may recommend the patient attend cardiac rehabilitation.
Nice to Know:
While still hospitalized, the patient may get to know members of the cardiac rehabilitation team. Cardiac rehabilitation services can involve many health care providers, including:
• Doctors, including the family doctor, a heart specialist or cardiologist, and a surgeon.
• Nurses
• Exercise specialists
• Physical and occupational therapists
• Dietitians
• Psychologists or other behavior therapists
Most patients suspected of having suffered an acute heart attack are admitted to a hospital's coronary care unit (CCU). The CCU is intended to be a quiet, calm, and restful area in which patients can be further evaluated and closely monitored. A specially trained nurse who works with doctors and other members of the medical team provides individualized care. Visiting hours are usually restricted.
The length of stay in the CCU varies, depending on :
• Whether or not the diagnosis of a heart attack is confirmed
• The severity of the heart attack
• The presence and severity of associated complications
A patient with a heart attack without complications spends about two to three days in a CCU before being transferred to a step-down unit. A step-down unit offers less intensive care than the CCU but still permits continuous ECG monitoring to screen for abnormal heart rhythms or other complications. The patient usually goes home five to seven days after hospital admission.
What Are The Goals Of Care In The CCU?
Care in the CCU focuses on:
• Relief of chest pain and anxiety
• Further assessment (diagnostic tests) to confirm a diagnosis
• Limiting the size of the heart attack and the area of heart muscle that dies
• Reducing the work of the heart
• Identifying, preventing, and treating complications from the heart attack
In the CCU:
• Care for the patient begun in the emergency setting continues
• Additional diagnostic tests are ordered
• Doctors determine appropriate medical-surgical intervention.
• The patient's level of activity and diet is restricted
Diet And Activity Levels
Additional precautions taken during the stay in the CCU and step-down unit, include
• Restricting the diet
For the first 24 hours, the patient is placed on a clear liquid diet to reduce the possibility of aspiration due to nausea and vomiting. A healthy food plan, including complex carbohydrates and fiber-rich foods, is later introduced. All individuals who have suffered a heart attack need to permanently adopt a healthy diet.
• Limiting activity levels
All patients are initially placed on bed rest. Patients who are stable, free of pain, and free of complications are sometimes to get out of bed to use the commode. Patients who remain free of complication often begin limited physical activities within 24 hours.
Progression Of Activity
Days 1-2
• Sitting up with feet dangling over the side of the bed
• Lifting and lowering of the arms, called range-of-motions exercises, to prevent muscle and joint stiffness and to prevent blood clots from forming in the legs
Days 3-4
• Bathing and dressing while sitting on the bed or in a chair
• Taking short walks around the hospital room
• Taking supervised walks outside the hospital room
• Showering without shampooing hair (no raising of arms above head)
Days 5-7
• Walking about 600 feet three times a day
• Shampooing hair (activities with arms over the head)
• Climbing stairs with supervision
• Undergoing an exercise tolerance test
After several days in the hospital, a patient with an uncomplicated heart attack can go home. Physical activity is then gradually increased over the next three to six weeks. Doctors may recommend the patient attend cardiac rehabilitation.
Nice to Know:
While still hospitalized, the patient may get to know members of the cardiac rehabilitation team. Cardiac rehabilitation services can involve many health care providers, including:
• Doctors, including the family doctor, a heart specialist or cardiologist, and a surgeon.
• Nurses
• Exercise specialists
• Physical and occupational therapists
• Dietitians
• Psychologists or other behavior therapists
WEIGHT-BASED HEPARIN DOSING
INITIAL THERAPY - Bolus 60-80 units/ Kg
- Infusion 14-18 units/kg/hr
ADJUSTMENTS
aPTT<40 - 2000 units IV bolus, increase infusion by 2 units/kg/hr aPTT 40-44 - increase infusion by 1 unit/kg/hr aPTT 45-70 - no change aPTT 71-80 - decrease infusion by 1 unit/kg/hr aPTT 81-90 - hold for 0.5 hour - decrease infusion by 2 units/kg/hr aPTT >90 - hold for 1 hour
- decrease infusion by 3 units/kg/hr
NOTE: drain aPTT 6 hours after any bolus or change in infusion rate
- Infusion 14-18 units/kg/hr
ADJUSTMENTS
aPTT<40 - 2000 units IV bolus, increase infusion by 2 units/kg/hr aPTT 40-44 - increase infusion by 1 unit/kg/hr aPTT 45-70 - no change aPTT 71-80 - decrease infusion by 1 unit/kg/hr aPTT 81-90 - hold for 0.5 hour - decrease infusion by 2 units/kg/hr aPTT >90 - hold for 1 hour
- decrease infusion by 3 units/kg/hr
NOTE: drain aPTT 6 hours after any bolus or change in infusion rate
Friday, April 30, 2010
CARDIAC DIET
The cardiac diet is often prescribed for people who are at imminent risk of a heart attack. The cardiac diet is a healthy eating plan to follow, even if a person does not have any of these health conditions, and may be followed as a preventative management program or as part of a heart healthy treatment plan.
When the cardiac diet is prescribed as part of a treatment plan, it is often individualized for the patient by a dietician and follows basic guidelines that promote good cardiac health.
1. Reduce the intake of food which contains animal fat.
2. Use trans fat free margarine instead of butter
3. Read labels and note the amount of trans fat contained in the food item, it should be “0″
4. Eat more fruits and vegetables
5. Reduce sodium intake.
6. Add fish to the diet
7. Eliminate caffeine
REDUCE FAT INTAKE
A key component in the cardiac diet is reducing the intake of harmful fats. Eliminating all fat is not healthy. It is important to understand what foods contain healthy fat and which foods contain fat that harms the arteries.
Polyunsaturated fats: This is a healthy type of fat that should be included in the diet. This type of fat can be found in fish and grain products.
Monounsaturated fats: These fats lower artery clogging cholesterol levels. They can be found in nuts, avocados, and olive oil.
Saturated fats: This type of harmful fat is found in meat, cheese, coconut oil and palm kernel oil.
Tran’s fat: These fats are chemically engineered and are used to hydrogenate oils. This process gives foods a longer shelf life, but they are not processed well in the body. These fats are found in packaged food items as well as many fried foods from fast food restaurants.
RED MEAT
Limit meat to 3-4 times per week.
Choose leaner cuts of meat like sirloin or round.
Choose meats that are at least 90% lean.
Make sure to rim away visible excess fat before cooking
FIBERS
Eating more fiber offers many health benefits. High fiber intake as part of the cardiac diet lower bad cholesterol levels in the body to increase health heart and reduce the risk of heart attacks. In addition to the cardiac benefits, fiber also aids digestion and reduces instances of constipation.
Women under 50 years of age should consume 25 grams of fiber per day, while those 51 and older should have 21 grams of daily fiber. Men under 50 years old should eat 38 grams of fiber and men over the age of 51 should take in 30 grams of fiber each day.
Fiber can be found in many foods
1. Whole grains
2. Legumes
3. Vegetables and fruits
4. Nuts and seeds
PRACTICE HEALTHY HABITS
In addition to following a healthy cardiac diet eating plan, there are other things you can do to keep your heart healthy.
One can enhance the effectiveness of this diet’s basic guidelines by not adding additional salt to foods, cooking with healthy oils such as olive oil, and exercising portion control to reduce caloric intake for weight management.
Get adequate exercise to keep your heart muscle strong and to lower cholesterol levels in the body. Getting 30 minutes of moderate exercise three to four times per week is usually adequate for heart health.
Avoid stress and develop coping skills to help you relax when stress is unavoidable. Being in a tense state is not good for cardiac health. Relaxation is also an important component in maintaining a healthy heart.
DIETARY RECOMMENDATIONS FOR CARDIAC PATIENTS
General Guidelines:
1. Lower the amount of total fat in your diet by eating fewer high fat foods. High fat foods often contain large amounts of saturated fat (most undesirable fat source).
2. Lower the amount of saturated fats while increasing the amount of polyunsaturated fat in the diet.
3. Lower cholesterol intake. Eat more fruit and vegetables and less animal products.
4. Eat more complex carbohydrates (starch and fiber). Foods high in complex carbohydrates are usually low in fat and contain no cholesterol.
5. Lose weight, if overweight, by decreasing the number of calories taken in and increasing the number of calories used.
To Eat Less Total Fat:
1. Within any food category, there are high fat and low fat items. Read labels to learn which foods are low in fat.
2. Sausage and most processed luncheon meats are high in fat and saturated fat.
3. Cream, sour cream, ice cream, butter, and many cheeses are high in fat and saturated fat.
To Eat Less Saturated Fat:
1. Steps you take to reduce total fat will also reduce saturated fat.
2. Most animal fats generally contain high proportions of saturated fat, whereas the fat in chicken and fish contains higher proportions of polyunsaturated fat.
3. The vegetable oils from palm kernel, coconut, and palm, and cocoa fat contain large proportions of saturated fat.
4. Vegetables oils with the highest proportions of polyunsaturated fat are safflower, sunflower, corn, soybean, and cottonseed oils.
5. Many margarine's are lower in saturated fat and higher in unsaturated fats than butter.
To Eat Less Cholesterol:
1. Cholesterol is found in high amounts of red meats, organ meats (liver, kidney, sweetbread, brain), and egg yolks. Shrimp is also high in cholesterol.
To Eat More Complex Carbohydrates:
1. Vegetables, fruits, cereal grains, dried peas and beans, rice, and pasta contain complex carbohydrates, little or no saturated fat, and no cholesterol.
To Help Lose Weight, If Overweight:
1. Fats are high in calories. Fat and oils supply 9 calories per gram as compared to protein, and carbohydrates, which supply only 4 calories per gram.
WHICH PEOPLE NEED TO ADHERE TO THE ABOVE ADVICE?
1. Everyone, the younger you start healthy eating habits the better.
2. Patients with a history for hypertension, congestive heart failure, coronary artery disease, stroke, peripheral vascular disease, or diabetes MUST make an extra effort to watch what they eat to lower their risk of atherosclerosis.
When the cardiac diet is prescribed as part of a treatment plan, it is often individualized for the patient by a dietician and follows basic guidelines that promote good cardiac health.
1. Reduce the intake of food which contains animal fat.
2. Use trans fat free margarine instead of butter
3. Read labels and note the amount of trans fat contained in the food item, it should be “0″
4. Eat more fruits and vegetables
5. Reduce sodium intake.
6. Add fish to the diet
7. Eliminate caffeine
REDUCE FAT INTAKE
A key component in the cardiac diet is reducing the intake of harmful fats. Eliminating all fat is not healthy. It is important to understand what foods contain healthy fat and which foods contain fat that harms the arteries.
Polyunsaturated fats: This is a healthy type of fat that should be included in the diet. This type of fat can be found in fish and grain products.
Monounsaturated fats: These fats lower artery clogging cholesterol levels. They can be found in nuts, avocados, and olive oil.
Saturated fats: This type of harmful fat is found in meat, cheese, coconut oil and palm kernel oil.
Tran’s fat: These fats are chemically engineered and are used to hydrogenate oils. This process gives foods a longer shelf life, but they are not processed well in the body. These fats are found in packaged food items as well as many fried foods from fast food restaurants.
RED MEAT
Limit meat to 3-4 times per week.
Choose leaner cuts of meat like sirloin or round.
Choose meats that are at least 90% lean.
Make sure to rim away visible excess fat before cooking
FIBERS
Eating more fiber offers many health benefits. High fiber intake as part of the cardiac diet lower bad cholesterol levels in the body to increase health heart and reduce the risk of heart attacks. In addition to the cardiac benefits, fiber also aids digestion and reduces instances of constipation.
Women under 50 years of age should consume 25 grams of fiber per day, while those 51 and older should have 21 grams of daily fiber. Men under 50 years old should eat 38 grams of fiber and men over the age of 51 should take in 30 grams of fiber each day.
Fiber can be found in many foods
1. Whole grains
2. Legumes
3. Vegetables and fruits
4. Nuts and seeds
PRACTICE HEALTHY HABITS
In addition to following a healthy cardiac diet eating plan, there are other things you can do to keep your heart healthy.
One can enhance the effectiveness of this diet’s basic guidelines by not adding additional salt to foods, cooking with healthy oils such as olive oil, and exercising portion control to reduce caloric intake for weight management.
Get adequate exercise to keep your heart muscle strong and to lower cholesterol levels in the body. Getting 30 minutes of moderate exercise three to four times per week is usually adequate for heart health.
Avoid stress and develop coping skills to help you relax when stress is unavoidable. Being in a tense state is not good for cardiac health. Relaxation is also an important component in maintaining a healthy heart.
DIETARY RECOMMENDATIONS FOR CARDIAC PATIENTS
General Guidelines:
1. Lower the amount of total fat in your diet by eating fewer high fat foods. High fat foods often contain large amounts of saturated fat (most undesirable fat source).
2. Lower the amount of saturated fats while increasing the amount of polyunsaturated fat in the diet.
3. Lower cholesterol intake. Eat more fruit and vegetables and less animal products.
4. Eat more complex carbohydrates (starch and fiber). Foods high in complex carbohydrates are usually low in fat and contain no cholesterol.
5. Lose weight, if overweight, by decreasing the number of calories taken in and increasing the number of calories used.
To Eat Less Total Fat:
1. Within any food category, there are high fat and low fat items. Read labels to learn which foods are low in fat.
2. Sausage and most processed luncheon meats are high in fat and saturated fat.
3. Cream, sour cream, ice cream, butter, and many cheeses are high in fat and saturated fat.
To Eat Less Saturated Fat:
1. Steps you take to reduce total fat will also reduce saturated fat.
2. Most animal fats generally contain high proportions of saturated fat, whereas the fat in chicken and fish contains higher proportions of polyunsaturated fat.
3. The vegetable oils from palm kernel, coconut, and palm, and cocoa fat contain large proportions of saturated fat.
4. Vegetables oils with the highest proportions of polyunsaturated fat are safflower, sunflower, corn, soybean, and cottonseed oils.
5. Many margarine's are lower in saturated fat and higher in unsaturated fats than butter.
To Eat Less Cholesterol:
1. Cholesterol is found in high amounts of red meats, organ meats (liver, kidney, sweetbread, brain), and egg yolks. Shrimp is also high in cholesterol.
To Eat More Complex Carbohydrates:
1. Vegetables, fruits, cereal grains, dried peas and beans, rice, and pasta contain complex carbohydrates, little or no saturated fat, and no cholesterol.
To Help Lose Weight, If Overweight:
1. Fats are high in calories. Fat and oils supply 9 calories per gram as compared to protein, and carbohydrates, which supply only 4 calories per gram.
WHICH PEOPLE NEED TO ADHERE TO THE ABOVE ADVICE?
1. Everyone, the younger you start healthy eating habits the better.
2. Patients with a history for hypertension, congestive heart failure, coronary artery disease, stroke, peripheral vascular disease, or diabetes MUST make an extra effort to watch what they eat to lower their risk of atherosclerosis.
Sunday, April 4, 2010
GOAL
I find it hard to believe that there is too little information one could get about Davao Regional Hospital in the internet, considering its popularity among the people of Davao and its wide service coverage in terms of land area. I can't even find its logo using Google Search. All we could see are pictures of DRH in the past. What about now? Our hospital has evolved for the better. It's about time to upload new and improved photos of DRH. It's about time to extend the services that DRH can offer through the cyber-space.
The official DRH website is yet to be finished. Until then, we will be providing relevant and up-to-date information about DRH through the world wide web with the use of this blogspot with the permission of our superiors. Our short-term goal is to be able to provide accurate and useful data related to healthcare, medicine, diagnostics and comptech support based on the demands of those who thirst for more knowledge. Our long-term goal... highlight the Davao Regional Hospital in Google Map as a Center of Excellence in Healthcare. Google's aerial photos of Tagum City ain't finished yet. The spot where our workplace is located cannot be zoomed yet to show a more detailed view. Google team, may you grant our simple request.
Our future posts will be based on your demands dear readers and subscribers. Feel free to send in your requests.
The official DRH website is yet to be finished. Until then, we will be providing relevant and up-to-date information about DRH through the world wide web with the use of this blogspot with the permission of our superiors. Our short-term goal is to be able to provide accurate and useful data related to healthcare, medicine, diagnostics and comptech support based on the demands of those who thirst for more knowledge. Our long-term goal... highlight the Davao Regional Hospital in Google Map as a Center of Excellence in Healthcare. Google's aerial photos of Tagum City ain't finished yet. The spot where our workplace is located cannot be zoomed yet to show a more detailed view. Google team, may you grant our simple request.
Our future posts will be based on your demands dear readers and subscribers. Feel free to send in your requests.
Wednesday, March 31, 2010
NORMAL VALUES
Arterial Blood Gases (ABGs) include:
* pH (norm 7.35-7.45)
* PaO2 (norm 80-100 mmHg)
*PaCO2 (norm 35-45 mmHg)
*HCO3 (norm 22-26 mEq/L)
*BE Base Excess (norm -2 to +2 mEq/L)
*SaO2 O2 saturation (norm 95-98%)
Vital Signs: normal
*T (96.6-99.3 F or 35.9-37.4 C)
*R (adults 12-18 CPM, infants 40-60 CPM)
*P (adults 60-100 BPM, infants 120-160 BPM)
*BP (young and middle-aged adults 120/80, older adults 140/80)
Electrolytes:
*Na (135-145 mEq/L)
*K (3.5-5mEq/L)
*Ca (9-10.5 mg/dl)
*Cl (90-110 mEq/L)
*Phosphorous (3-4.5 mg/dl)
Hematology:
Bleeding Time (1-9 minutes)
ESR (male-up to 15 mm/hr, female-up to 20 mm/hr)
Hct (male-< 47%, female-<42%)
Hgb (male 14-18 g/dl , female 12-16 g/dl)
Plt (150,000-450,000)
Protime (11-12 secs)
RBC (male 4.7-6.1 M/cu mm, female 4.2-5.4 M/ cu mm)
WBC (5,000-10,000 / cu mm)
Thyroid:
T3 (75-220 ug/dl)
T4 (4-11 ug/dl)
Others:
Cholesterol Level(<200 mg/dl)
Crea (.5-1.5 mg/dl)
Ig E (<.55 mg/dl)
Ig M (55-375 mg/dl)
Lead (<20 ug/dl)
SGOT/AST (8-20 U/L)
SGPT/ALT (8-20 U/L)
* pH (norm 7.35-7.45)
* PaO2 (norm 80-100 mmHg)
*PaCO2 (norm 35-45 mmHg)
*HCO3 (norm 22-26 mEq/L)
*BE Base Excess (norm -2 to +2 mEq/L)
*SaO2 O2 saturation (norm 95-98%)
Vital Signs: normal
*T (96.6-99.3 F or 35.9-37.4 C)
*R (adults 12-18 CPM, infants 40-60 CPM)
*P (adults 60-100 BPM, infants 120-160 BPM)
*BP (young and middle-aged adults 120/80, older adults 140/80)
Electrolytes:
*Na (135-145 mEq/L)
*K (3.5-5mEq/L)
*Ca (9-10.5 mg/dl)
*Cl (90-110 mEq/L)
*Phosphorous (3-4.5 mg/dl)
Hematology:
Bleeding Time (1-9 minutes)
ESR (male-up to 15 mm/hr, female-up to 20 mm/hr)
Hct (male-< 47%, female-<42%)
Hgb (male 14-18 g/dl , female 12-16 g/dl)
Plt (150,000-450,000)
Protime (11-12 secs)
RBC (male 4.7-6.1 M/cu mm, female 4.2-5.4 M/ cu mm)
WBC (5,000-10,000 / cu mm)
Thyroid:
T3 (75-220 ug/dl)
T4 (4-11 ug/dl)
Others:
Cholesterol Level(<200 mg/dl)
Crea (.5-1.5 mg/dl)
Ig E (<.55 mg/dl)
Ig M (55-375 mg/dl)
Lead (<20 ug/dl)
SGOT/AST (8-20 U/L)
SGPT/ALT (8-20 U/L)
Subscribe to:
Comments (Atom)



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}